This website is best viewed using the horizontal display on your tablet device.
- INDICATIONS

ABRAXANE® is indicated for the treatment of breast cancer after failure of combination chemotherapy for metastatic disease or relapse within 6 months of adjuvant chemotherapy. Prior therapy should have included an anthracycline unless clinically contraindicated.
ABRAXANE® is indicated for the first-line treatment of locally advanced or metastatic non–small cell lung cancer, in combination with carboplatin, in patients who are not candidates for curative surgery or radiation therapy.
ABRAXANE® is indicated for the first-line treatment of patients with metastatic adenocarcinoma of the pancreas, in combination with gemcitabine.
- FULL PRESCRIBING INFORMATION INCLUDING BOXED WARNING
- PATIENT INFORMATION
- PATIENT SITES
- BMS ACCESS SUPPORT
- BMS RESOURCES
THIS SITE IS INTENDED FOR U.S. HEALTHCARE PROFESSIONALS ONLY.
This website is best viewed using the vertical display on your mobile device.
THIS SITE IS INTENDED FOR U.S. HEALTHCARE PROFESSIONALS ONLY.
DELIVER THE BRIGHT CHOICE
A distinctive taxane: The first nanoparticle albumin-bound paclitaxel1,2
THIS SITE IS INTENDED FOR U.S. HEALTHCARE PROFESSIONALS ONLY.
DELIVER THE BRIGHT CHOICE
A distinctive taxane: The first nanoparticle albumin-bound paclitaxel1,2
THIS SITE IS INTENDED FOR U.S HEALTHCARE PROFESSIONALS ONLY.
WHEN IS CHEMOTHERAPY AN APPROPRIATE TREATMENT CHOICE
IN HER2-NEGATIVE METASTATIC BREAST CANCER (MBC)?3,4
- Triple negative breast cancer (TNBC)
- Hormone receptor (HR) + and hormone refractory/resistant disease
- Visceral metastases
When selecting chemotherapy in patients with MBC, what characteristics or poor prognostic factors are considered?
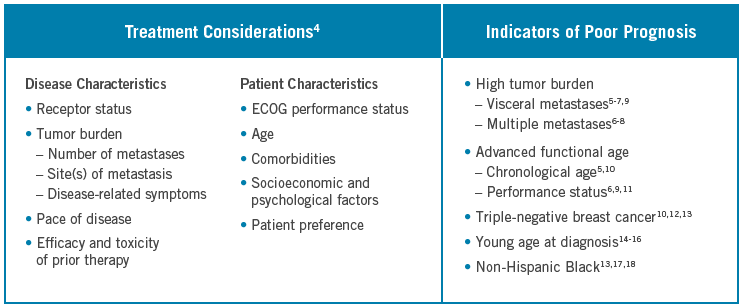
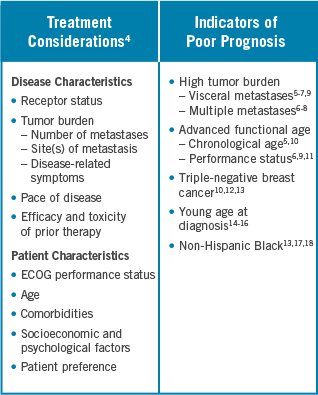
ECOG=Eastern Cooperative Oncology Group.

Learn More: ABRAXANE’s Phase III Trial Designed to Assess Response Rates
in MBC Patients, Including Those With Poor Prognostic Factors

PATIENTS WHO HAVE MBC WITH VISCERAL AND MULTIPLE
METASTASES OFTEN HAVE LESS FAVORABLE OUTCOMES
There is lower median survival time for patients who develop visceral metastases vs nonvisceral metastases5,a


- A retrospective database analysis of 111 women at a single center in Canada between 2005 and 2007 found that about 67%-73% of patients with metastatic breast cancer (MBC) developed visceral metastases.19 A retrospective analysis of 6 clinical studies between 1983 and 2001 (N=640) found that in 57%-74% of patients, visceral metastases developed as the dominant metastatic site9
- Further studies demonstrate that up to 85% of patients will develop visceral metastases at some point in the course of their disease7,20-22
- Visceral metastases are associated with more aggressive MBC compared with nonvisceral metastases; patients tend to have worse outcomes5
The number of metastatic sites is associated with more aggressive MBCa
- The presence of multiple metastatic lesions or sites is associated with poor prognosis in patients with MBC6
- Patients with MBC who present metastases at ≥3 sites are likely to have a comparatively less favorable outcome than those with ≤2 metastatic sites8
Univariate survival analysis from a retrospective database of 346 patients diagnosed with MBC after first recurrence between 1970 and 1991.
All patients had undergone surgery for primary breast cancer and may have received radiation, hormonal therapy, and/or chemotherapy for metastatic disease.5
THERE IS LOWER MEDIAN SURVIVAL TIME FOR PATIENTS WITH INCREASING NUMBER OF METASTATIC SITES6,a
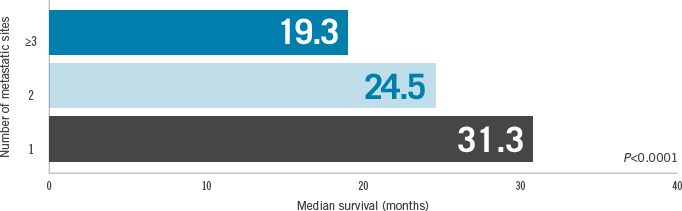
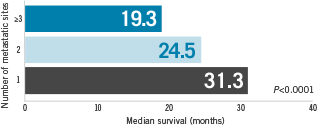
Univariate survival analysis of 1430 patients from 8 consecutive prospective trials conducted between 1977 and 1992 of anthracycline-based first-line chemotherapy in MBC.
CLOSE THE TAB
Learn More: Majority of Patients From ABRAXANE MBC Phase III Trial
Had Multiple and Visceral Metastases
BASELINE PATIENT CHARACTERISTICS IN THE ABRAXANE PHASE III STUDY
Study design
Multicenter, 1:1 randomized, Phase III study comparing ABRAXANE 260 mg/m2 IV Q3W with paclitaxel injection 175 mg/m2 IV Q3W in 460 patients with MBC. The primary efficacy endpoint was recTLRR. recTLRR was based on independent radiologic assessment of target lesions reconciled with investigator-reported responses for the first 6 cycles of therapy. The recTLRR was lower than the investigator-reported response rates, which are based on all cycles of therapy. The secondary endpoints were time to disease progression and overall survival.
IV=intravenously; PS=performance status; Q3W=every 3 weeks; recTLRR=reconciled target lesion response rate.
PHASE III RIGOROUS TUMOR RESPONSE ENDPOINT: recTLRR
- The primary efficacy endpoint: reconciled target lesion response rate (recTLRR)
- recTLRR was based on independent radiologic assessment of tumor responses
- recTLRR was reconciled with investigator-reported responses for the first 6 cycles of therapy
- Secondary efficacy endpoints included time to disease progression and overall survival, among other measures24
- An exploratory analysis was conducted for overall survival to evaluate the subgroup of patients receiving ABRAXANE as second-line or later therapy
Patients who completed 6 cycles of ABRAXANE therapy and did not progress were able to continue treatment at the investigator's discretion.24
CLOSE THE TABRECOMMENDATIONS FOR METASTATIC BREAST CANCER PATIENTS WITH VISCERAL METASTASES
The predominance of visceral metastases in the Phase III study is consistent with the National Comprehensive Cancer Network® (NCCN®) recommended* patient population for albumin-bound paclitaxel (ABRAXANE).3
NCCN Guidelines® (V.6.2020) recommend albumin-bound paclitaxel as Category 2A.
CLOSE THE TAB
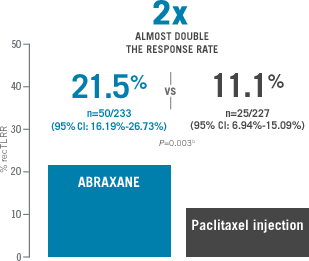
Learn More: ABRAXANE Delivered Almost Double the Response Rates vs
Paclitaxel Injection in MBC
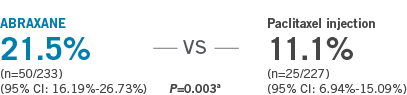
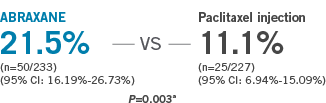
WHEN RESPONSE RATES MATTER, CHOOSE ABRAXANE
Primary endpoint was response rate in ITT population based on reconciled investigator and independent radiologic assessments of target lesions through cycle 6 (recTLRR)a ABRAXANE 260 mg/m2 IV Q3W vs paclitaxel injection 175 mg/m2 IV Q3W

ITT=intent-to-treat.
recTLRR was the prospectively defined, protocol-specific endpoint, based on independent radiologic assessment of tumor responses reconciled with investigator responses (which also included clinical information) for the first 6 cycles of therapy. The recTLRR was lower than the investigator-reported response rates, which are based on all cycles of therapy.
From Cochran-Mantel-Haenszel test stratified by first-line vs > first-line therapy.
IN RELAPSED OR REFRACTORY METASTATIC BREAST CANCER,
RESPONSE RATES ARE AN IMPORTANT MEASURE
recTLRR: ABRAXANE vs paclitaxel injection for patients who failed combination chemotherapy or relapsed within 6 months of adjuvant chemotherapy (indicated population)
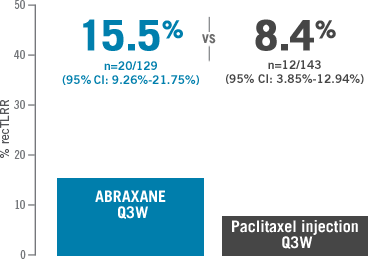
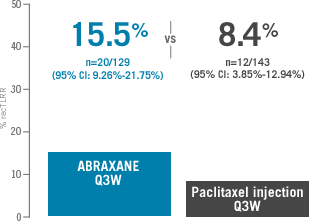
Prior therapy included an anthracycline unless clinically contraindicated.
MEDIAN TIME TO FIRST CONFIRMED RECONCILED RESPONSE WITH ABRAXANE (EXPLORATORY ENDPOINT FOR ITT)24,a
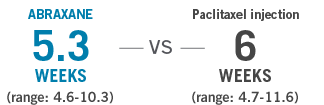
Analysis Limitations: Time to first reconciled response was an exploratory endpoint that was not powered to determine a treatment difference.

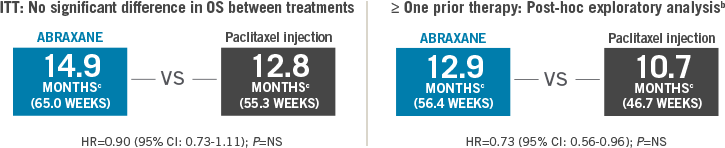
Compare Median Overall Survival (OS) Data: ABRAXANE vs Paclitaxel Injection
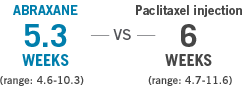
MEDIAN OVERALL SURVIVAL DATA:
ABRAXANE VS PACLITAXEL INJECTION23
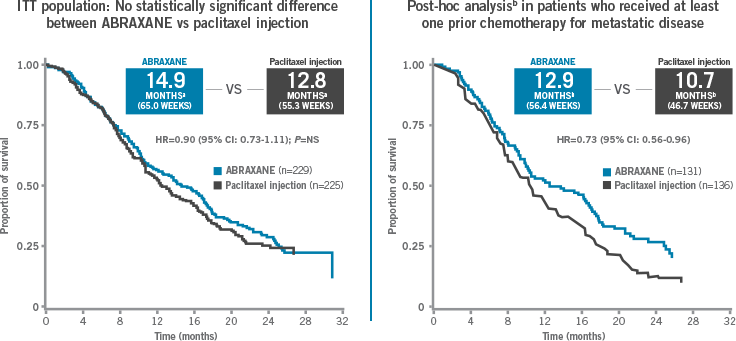
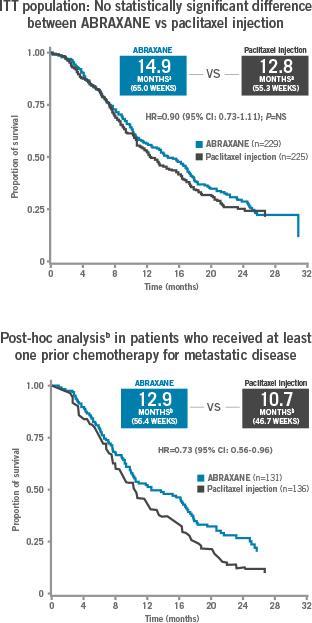
Median overall survival was measured in weeks and converted to months (assuming 4.348125 weeks in 1 Gregorian month).
Analysis Limitations: A post-hoc exploratory analysis should not be interpreted to determine a treatment difference between arms in this selected subgroup because of potential selection bias, insufficient sample size, and a higher probability of making a false positive finding.
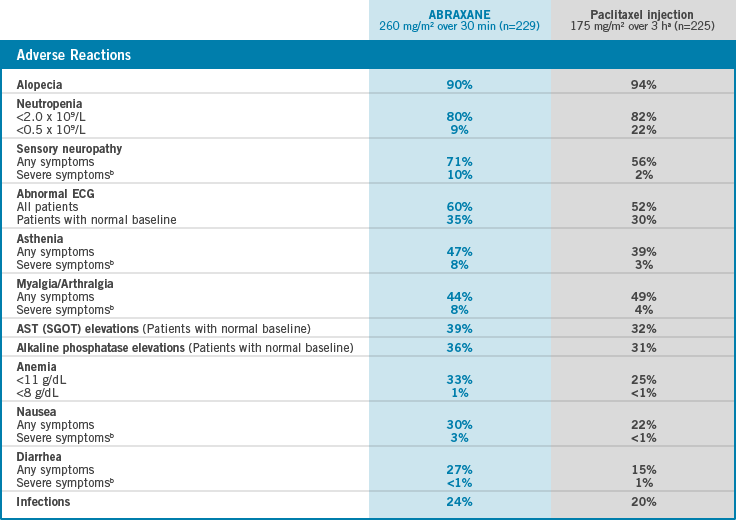
OBSERVED SAFETY PROFILE
MOST COMMON ADVERSE EVENTS IN >20% OF PATIENTS
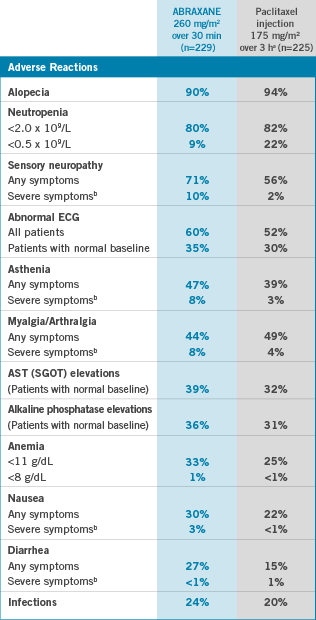
AST=aspartate aminotransferase; ECG=electrocardiogram;
SGOT=serum glutamic-oxaloacetic transaminase.
Paclitaxel injection patients received premedication.
Severe events are defined as at least Grade 3 toxicity.
OBSERVED SAFETY PROFILE
ADVERSE EVENTS IN A PHASE III CLINICAL TRIAL
Frequencya of important treatment-emergent adverse events in the randomized study of an every-3-week schedule
Frequencya of important treatment-emergent adverse events in the randomized study of an every-3-week schedule
PERCENTAGE OF PATIENTS
ABRAXANE
260 mg/m2 over 30 min (n=229)
Paclitaxel injection 175 mg/m2 over 3 hb (n=225)
| HEMATOLOGIC | ||
| BONE MARROW | ||
| Neutropenia | ||
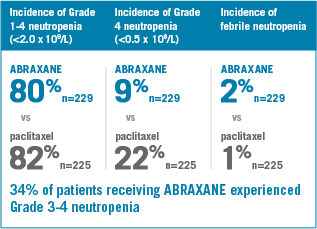
| <2.0 x 109/L | 80 | 82 |
| <0.5 x 109/L (Grade 4) | 9 | 22 |
| Thrombocytopenia | ||
| <100 x 109/L | 2 | 3 |
| <50 x 109/L (Grade ≥3) | <1 | <1 |
| Anemia | ||
| <11 g/dL | 33 | 25 |
| <8 g/dL (Grade ≥3) | 1 | <1 |
| Infections | 24 | 20 |
| Febrile Neutropenia | 2 | 1 |
| Neutropenic Sepsis | <1 | <1 |
| Bleeding | 2 | 2 |
| NONHEMATOLOGIC | ||
| HYPERSENSITIVITY REACTIONc | ||
| All | 4 | 12 |
| Severed | 0 | 2 |
| CARDIOVASCULAR | ||
| Vital Sign Changes During Administration | ||
| Bradycardia | <1 | <1 |
| Hypotension | 5 | 5 |
| Severe Cardiovascular Eventsd | 3 | 4 |
| ABNORMAL ECG | ||
| All Patients | 60 | 52 |
| Patients With Normal Baseline | 35 | 30 |
| RESPIRATORY | ||
| Cough | 7 | 6 |
| Dyspnea | 12 | 9 |
| SENSORY NEUROPATHY | ||
| Any Symptoms | 71 | 56 |
| Severe Symptomsd | 10 | 2 |
| MYALGIA/ARTHRALGIA | ||
| Any Symptoms | 44 | 49 |
| Severe Symptomsd | 8 | 4 |
| ASTHENIA | ||
| Any Symptoms | 47 | 39 |
| Severe Symptomsd | 8 | 3 |
| FLUID RETENTION/EDEMA | ||
| Any Symptoms | 10 | 8 |
| Severe Symptomsd | 0 | <1 |
| GASTROINTESTINAL | ||
| Nausea | ||
| Any Symptoms | 30 | 22 |
| Severe Symptomsd | 3 | <1 |
| Vomiting | ||
| Any Symptoms | 18 | 10 |
| Severe Symptomsd | 4 | 1 |
| Diarrhea | ||
| Any Symptoms | 27 | 15 |
| Severe Symptomsd | <1 | 1 |
| Mucositis | ||
| Any Symptoms | 7 | 6 |
| Severe Symptomsd | <1 | 0 |
| ALOPECIA | 90 | 94 |
| HEPATIC (PATIENTS WITH NORMAL BASELINE) | ||
| Bilirubin Elevations | 7 | 7 |
| Alkaline Phosphatase Elevations | 36 | 31 |
| AST (SGOT) Elevations | 39 | 32 |
| INJECTION-SITE REACTION | <1 | 1 |
NCI=National Cancer Institute.
Based on worst grade by NCI Common Terminology Criteria for Adverse Events (CTCAE) version 2.
Paclitaxel injection patients received premedication.
Includes treatment-related events related to hypersensitivity (eg, flushing, dyspnea, chest pain, hypotension) that began on a day of dosing.
Severe events are defined as at least Grade 3 toxicity.
CLOSE THE TAB
Download the “Preparing for My Treatment” Brochure: Help Your
Patients With MBC Get Ready for Their Medical Appointments

UNDERSTANDING AND ADDRESSING NEUROPATHY
ABRAXANE PHASE III MBC TRIAL
71% of 229 patients who received ABRAXANE developed Grades 1-3 sensory neuropathy (no Grade 4 was reported)
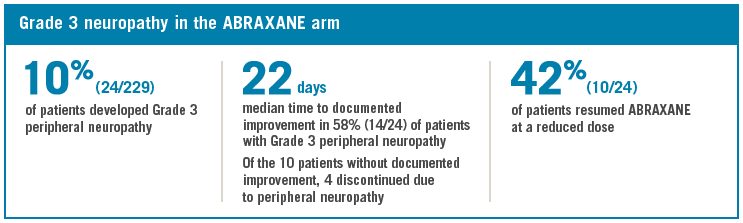
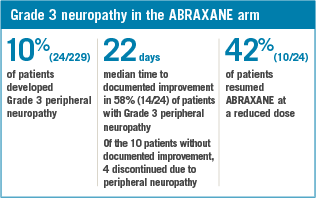
- The frequency and severity of sensory neuropathy increased with cumulative doses of ABRAXANE
- 3% of patients (7/229) discontinued treatment with ABRAXANE due to sensory neuropathy
- Only 1 incident of motor neuropathy (Grade 2) was observed in either arm of the controlled trial

Learn About Dose Modifications for Treatment-related Neuropathy
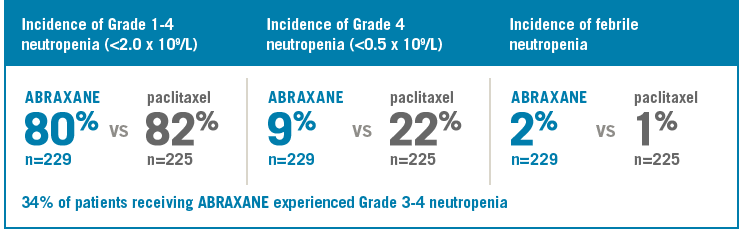
UNDERSTANDING AND ADDRESSING NEUTROPENIA
ABRAXANE PHASE III MBC TRIAL
Learn About Dose Modifications For Treatment-related Neutropenia
UNDERSTANDING DURATION AND DOSING
ABRAXANE PHASE III MBC TRIAL
Patients treated with ABRAXANE received a median of 6 cycles of therapy

- The primary endpoint, recTLRR, was the evaluation of responses achieved in the first 6 cycles of therapy
FDA-approved dose and schedule for ABRAXANE in metastatic breast cancer:
- Administer intravenously at a dose of 260 mg/m2
- Recommended schedule is once every 3 weeks
- Administer over 30 minutes
- Premedication to prevent hypersensitivity reactions is generally not needed prior to the administration of ABRAXANE. Premedication may be needed in patients who have had prior hypersensitivity reactions to ABRAXANE. Patients who experience a severe hypersensitivity reaction to ABRAXANE should not be rechallenged with this drug
Reconstitution Video
DOSE MODIFICATIONS
FOR PATIENTS WITH HEPATIC IMPAIRMENT
Recommendations for starting dose in patients with hepatic impairment
SGOT (AST) LEVELS
<10 x ULN
AND
BILIRUBIN LEVELS
> ULN TO ≤1.5 x ULN
SGOT (AST) LEVELS
<10 x ULN
AND
BILIRUBIN LEVELS
> 1.5 TO ≤3 x ULN
SGOT (AST) LEVELS
<10 x ULN
AND
BILIRUBIN LEVELS
> 3 TO ≤5 x ULN
SGOT (AST) LEVELS
>10 x ULN
AND
BILIRUBIN LEVELS
>5 x ULN
Mild
- No dose adjustment is necessary for patients with mild hepatic impairment
- Do not administer ABRAXANE to patients with total bilirubin >5 x ULN or AST >10 x ULN
- Dosage recommendations are for the first course of therapy. The need for further dose adjustments in subsequent courses should be based on individual tolerance
Moderate
- Do not administer ABRAXANE to patients with total bilirubin >5 x ULN or AST >10 x ULN
- Dosage recommendations are for the first course of therapy. The need for further dose adjustments in subsequent courses should be based on individual tolerance
Severe
- Do not administer ABRAXANE to patients with total bilirubin >5 x ULN or AST >10 x ULN
- Dosage recommendations are for the first course of therapy. The need for further dose adjustments in subsequent courses should be based on individual tolerance
- Do not administer ABRAXANE to patients with total bilirubin >5 x ULN or AST >10 x ULN
ABRAXANE dose



ILLUSTRATIVE PURPOSES ONLY
A dose increase to 260 mg/m2 in subsequent courses should be considered if the patient tolerates the reduced dose for 2 cycles.
DOSING FOR YOUR PATIENTS
WHO EXPERIENCE SENSORY NEUROPATHY
ABRAXANE dose-modification schedule for neuropathy
Mild to Moderate
The occurrence of Grade 1 or 2 sensory neuropathy does not generally require dose modification
- In the Phase III ABRAXANE MBC clinical trial, sensory neuropathy with any symptoms occurred in 71% of patients receiving ABRAXANE 260 mg/m2 over 30 minutes; sensory neuropathy with severe symptoms (defined as ≥ Grade 3 toxicity) occurred in 10% of patients receiving ABRAXANE
Severe
If ≥ Grade 3 sensory neuropathy develops, hold until resolution to Grade 1 or 2 followed by a dose reduction for all subsequent courses of ABRAXANE
- In the Phase III ABRAXANE MBC clinical trial, sensory neuropathy with any symptoms occurred in 71% of patients receiving ABRAXANE 260 mg/m2 over 30 minutes; sensory neuropathy with severe symptoms (defined as ≥ Grade 3 toxicity) occurred in 10% of patients receiving ABRAXANE
Recurrent
If severe (≥ Grade 3) neuropathy is recurrent, hold treatment until resolution to Grade 1 or 2, then reduce dose from 220 mg/m2 to 180 mg/m2 for all subsequent courses
- In the Phase III ABRAXANE MBC clinical trial, sensory neuropathy with any symptoms occurred in 71% of patients receiving ABRAXANE 260 mg/m2 over 30 minutes; sensory neuropathy with severe symptoms (defined as ≥ Grade 3 toxicity) occurred in 10% of patients receiving ABRAXANE
- Do not administer ABRAXANE to patients with total bilirubin >5 x ULN or AST >10 x ULN
ABRAXANE dose


ILLUSTRATIVE PURPOSES ONLY
DOSING FOR YOUR PATIENTS
WHO EXPERIENCE NEUTROPENIA
ABRAXANE dose-modification schedule for neutropenia
Mild to Moderate
- If neutropenia is mild or moderate (Grade 1 or 2), no dose reduction is needed
- ABRAXANE has a dose-reduction schedule for patients who experience severe neutropenia
- Monitor for myelotoxicity by performing complete blood cell counts frequently, including prior to dosing on Day 1
- In the Phase III ABRAXANE MBC clinical trial, neutropenia (<2.0 x 109/L) occurred in 80% of patients receiving ABRAXANE 260 mg/m2 over 30 minutes; neutropenia (<0.5 x 109/L) occurred in 9% of patients receiving ABRAXANE
Severe
- If neutropenia is severe (neutrophils <500 cells/mm3 for 7 days or longer), reduce dose from 260 mg/m2 to 220 mg/m2 for subsequent courses
- ABRAXANE has a dose-reduction schedule for patients who experience severe neutropenia
- Monitor for myelotoxicity by performing complete blood cell counts frequently, including prior to dosing on Day 1
- In the Phase III ABRAXANE MBC clinical trial, neutropenia (<2.0 x 109/L) occurred in 80% of patients receiving ABRAXANE 260 mg/m2 over 30 minutes; neutropenia (<0.5 x 109/L) occurred in 9% of patients receiving ABRAXANE
Recurrent
- If severe neutropenia is recurrent, reduce dose from 220 mg/m2 to 180 mg/m2 for subsequent courses
- ABRAXANE has a dose-reduction schedule for patients who experience severe neutropenia
- Monitor for myelotoxicity by performing complete blood cell counts frequently, including prior to dosing on Day 1
- In the Phase III ABRAXANE MBC clinical trial, neutropenia (<2.0 x 109/L) occurred in 80% of patients receiving ABRAXANE 260 mg/m2 over 30 minutes; neutropenia (<0.5 x 109/L) occurred in 9% of patients receiving ABRAXANE
- Do not administer ABRAXANE to patients with total bilirubin >5 x ULN or AST >10 x ULN
ABRAXANE dose

ILLUSTRATIVE PURPOSES ONLY
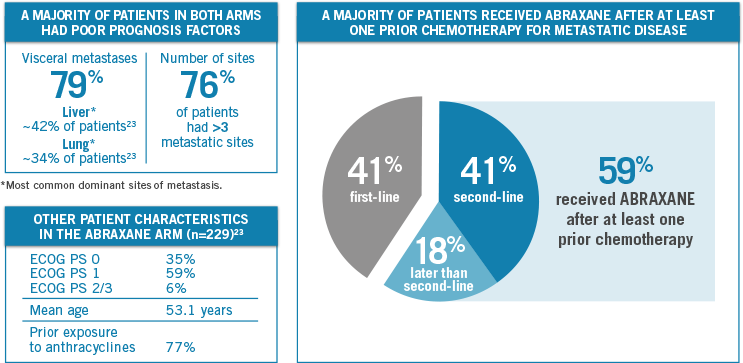
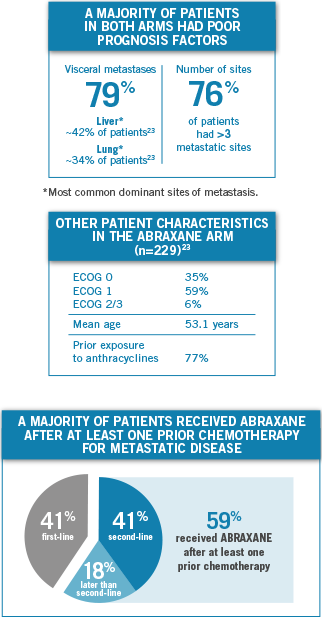
THE MAJORITY OF PATIENTS IN BOTH ARMS HAD POOR PROGNOSTIC FACTORS
- 79%
had visceral metastases - 76%
>3 sites of metastases
ABRAXANE ALMOST DOUBLED THE RESPONSE RATE (recTLRR) VS PACLITAXEL IN THE ITT POPULATION
- Indication population:
15.5% (n=20/129 [95% CI: 9.26%-21.75%]) vs
8.4% (n=12/143 [95% CI: 3.85%-12.94%])
From Cochran-Mantel-Haenszel test stratified by first-line vs > first-line therapy.
MEDIAN OVERALL SURVIVAL23
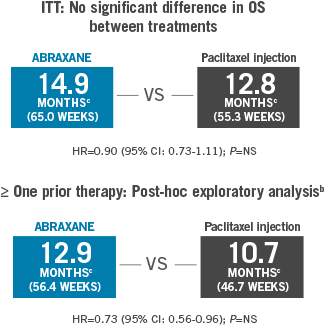
Analysis Limitations: A post-hoc exploratory analysis should not be interpreted to determine a treatment difference between arms in this selected subgroup because of potential selection bias, insufficient sample size, and a higher probability of making a false positive finding.
Median overall survival was measured in weeks and converted to months (assuming 4.348125 weeks in 1 Gregorian month).
MOST COMMON AEs (≥20%)
- Alopecia
- Neutropenia
- Sensory Neuropathy
- Abnormal ECG
- Fatigue/Asthenia
- Myalgia/Arthralgia
- AST Elevations
- Alkaline Phosphatase Elevations
- Anemia
- Nausea
- Infections
- Diarrhea
Study design
Multicenter, 1:1 randomized, Phase III study comparing ABRAXANE 260 mg/m2 IV Q3W with paclitaxel injection 175 mg/m2 IV Q3W in 460 patients with MBC. The primary efficacy endpoint was recTLRR. recTLRR was based on independent radiologic assessment of target lesions reconciled with investigator-reported responses for the first 6 cycles of therapy. The recTLRR was lower than the investigator-reported response rates, which are based on all cycles of therapy. The secondary endpoints were time to disease progression and overall survival.

Healthcare Professional Resources
Gain Access to a Range of Valuable Resources


Patient Resources
Gain Access to a Range of Resources for Your MBC Patients